86 YR OLD MALE WITH DCMP( Dilated Cardiomyopathy) SECONDARY TO IHD( Ischemic Heart disease) WITH MAT (multifocal atrial tachycardia )WITH COPD .
86 YR OLD MALE WITH DCMP( Dilated Cardiomyopathy) SECONDARY TO IHD( Ischemic Heart disease) WITH MAT (multifocal atrial tachycardia )WITH COPD .
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : K. Supriya (9th semester)
Roll number : 53
86 YEAR OLD MALE PATIENT CAME TO THE CASUALITY ON 18 /10/21
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
Presenting complaints are :
▪️ c/o shortness of breath ( grade 4) acc to NYHA classification since 4 days
▪️ c/o orthopnea since 4 days
▪️ c/o fever since 1 day
# This patient was a farmer 18 years ago,he stopped his work as they sold out their land, during his life as a farmer he was a very active& talkative person and have very good relationships with family and friends even now,who wakes up at 5am goes to his work and used to have breakfast(rice& curry) at around 8am ,lunch (rice &curry) at 1pm ,he had mixed type of diet,which includes non veg more than veg (like more than 4 times in a week) and comes back his home at around 5pm and he usually used to have dinner(rice&curry) at around 7:30pm and goes to bed at 9pm. (He was a chronic smoker then)
11 years ago,he had a prick to his left foot,which developed into ulcer,that made him little depressed and bit irritated as it's not healing completely since then, but even now, he has very good relationships.(he stopped smoking ).His diet ,which included non veg more,before,limited to once in a week.
He is a Occasional alcoholic.
2years ago he had SOB associated with orthopnea .
That whole scenario is explained below in the form of HOPI
Patient was apparently assymptomatic 11 years back then he had a prick to his left foot and developed swelling and was taken to RMP and told he has infection and was brought to our hospital which was diagnosed with non healing ulcer after 1 week he was taken to Hyderabad for further evaluation and grafting was done and which was not successful and he got dressing regularly for next 6 months .
And for the next 6 years he didn't have any complaints, ulcer was healing acc to the attender .
2 years back patient had shortness of breath ( grade 4 , according to NYHA) ,associated with orthopnea ,was taken to Osmania hospital and was diagnosed with HFrEF with EF35% and was put on INJ LASIX and regular dressings was done for the next 2 years.
NYHA classification: SOB
Grade 1: on extremely severe exercise
Grade 2: on accustomed work
Grade 3: on routine activity
Grade 4 : at rest
From 4 days patient had not taken his regular medication
Not a K/C/O DM ,HTN ,ASTHMA, EPILEPSY
K/C/O COPD
Patient is a chronic smoker ( 5 cigarettes/ day or more )
and he stopped smoking since 10 years.
General Examination :
pallor present
No Icterus,
No cyanosis,
No clubbing,lymphaedonopathy,oedema
Vitals :
Temp-afebrile
PR-130bpm
RR-29 fpm
BP-110/60 MMHG
SPO2-97 @ ROOM AIR
GRBS - 149 mg/dl
Systemic Examination: CVS
Inspection :
Shape of the chest : elliptical (transverse diameter is more than AP diameter )
Symmetry: bilaterally symmetrical
Position of trachea : central
there is no precordial bulge ,
,no scars and sinuses ,no engorged veins
JVP raised
Palpation :
All inspectory findings are confirmed
Position of trachea is central
Apex beat -at left 6th intercostal space ( at mid clavicular line).
No thrills .
JVP raised .
Auscultation :
S1S2 HEARD
APEX BEAT,6th intercostal space at mcl
RS:
B/L INSPIRATORY CREPTS IN ISA,IAA
B/L EXPIRATORY WHEEZE IN IAA,ISA
P/A:
SOFT,NON TENDER
Bowel sounds +
CNS: NAD
CLINICAL IMAGES :





Provisional diagnosis:
HFrEF with EF 45% with COPD with Non healing ulcer of left foot
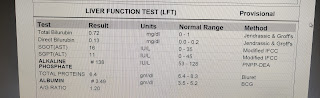
INVESTIGATIONS :
On 18/10/21 :








Links:
ECG:

On 19/10/21 :
Rtpcr negative


On 20/10/21
Serology negative

ECG : 20/10/21

On 21/10/21
APTT 33 sec
INR 1.11
PT 16 sec
TREATMENT GIVEN :
1.)Head end elevation upto 30°
2.)Fuild restriction upto 1 lit / day
3.)Salt restriction < 2.5 g/ day
4.)Inj Neomol 100 ML IV / if temp > 101° F
5.)Nebulisation with ipravent 6 th hrly and budecort 12 th hrly
6.)Inj pantop 40 MG /IV /OD
7.)Tab carvidelol 1.25 mg / po/od
8.)Inj Hydrocortisone 100 mg / iv stat
9.)Inj lasix 10 ampules ( 200 mg ) in 30 ml NS at 2 ml / hr
10.)Dressing for Left LL ulcer
11) Moniter vitals
CASE DISCUSSION DONE WITH -Dr .Vamshi Sir (PGY2).
SOAP NOTES : (obtained from Intern -Sai surya Sir)
AMC Bed 1
Unit I admission
SOAP notes Day 2
19/10 /21
S : decrease in SOB
No fever episode .
O : Pt is conscious ,coherent, cooperative
Pt is symptomatically improved
O/E
Pallor +
JVP +
PR 130 bpm
BP 100/70 mmHg
RR 28 cpm
Temp 98.6 F
CVS :
JVP elevated
Apex beat in 6 th ICS at MCL
S1 S2 heard
RS :
B/L INSPIRATORY CREPTS IN ISA,IAA
B/L EXPIRATORY WHEEZE IN IAA,ISA
P/A :
Soft , non tender
Bowel sounds +
CNS : NAD
A:
HFrEF with EF 45% secondary to CAD with COPD with Non healing ulcer of left foot since 10 yrs ( S/p : grafting ? )
With MAT ( Multifocal Atrial Tachycardia )
P:
1.)Head end elevation upto 30°
2)Oxygen supplementation .Maintain O2 at > 92%
3.)Fuild restriction upto 1 lit / day
4)Salt restriction < 2 g/ day
5)Inj Lasix infusion @ 1ml/hr
6.)Inj pantop 40 MG /IV /OD
7.)Tab carvidelol 1.25 mg / po/bd
8 am ......x ......8 pm
8) Tab Dolo 650 mg PO /SOS
9)Nebulisation with ipravent 6 th hrly and budecort 12 th hrly .
10.)Dressing for Left LL ulcer
11) Moniter vitals
12) Strict I/o charting
INJ lasix infusion 10 ampules in 30 ml NS
13) Tab Ecosprin AV /PO/ HS .....75/20
x ...........x..........8 pm
14) Inj Clexane 40 mg / sc / od
15) Inj hydrocort 100 mg / IV /TID
SOAP notes Day 3
20/10/21
Fever chart :

S: : decrease in SOB
No fever episode .
O : Pt is conscious ,coherent, cooperative
Pt has tachycardia
O/E
Pallor +
PR 105 bpm
BP 110/70 mmHg
RR 22 cpm
Temp 98.6 F
CVS :
Apex beat in 6 th ICS at MCL
S1 S2 heard
RS :
B/L INSPIRATORY CREPTS IN ISA,IAA
B/L EXPIRATORY WHEEZE IN IAA,ISA
P/A :
Soft , non tender
Bowel sounds +
CNS : NAD
A:
DCMP secondary to IHD With MAT ( Multifocal Atrial Tachycardia )
secondary to CAD with COPD with Non healing ulcer of left foot since 10 yrs ( S/p : grafting ? )
P:
1.)Head end elevation upto 30°
2)Oxygen supplementation .Maintain O2 at > 92%
3.)Fuild restriction upto 1 lit / day
4)Salt restriction < 2 g/ day
6.)Inj pantop 40 MG /IV /OD
7.)Tab carvidelol 3.125 mg / po/bd (increased from od to bd)
8 am ......x ......8 pm
8) Tab Dolo 650 mg PO /SOS
9)Nebulisation with ipravent 6 th hrly and budecort 12 th hrly .
10.)Dressing for Left LL ulcer
11) Moniter vitals
12) Strict I/o charting
13) Tab Ecosprin AV /PO/ HS .....75/20
x ...........x..........8 pm
14) Inj Clexane 40 mg / sc / od
15) Inj hydrocort 100 mg / IV /TID
Plan Any rate control agents to be added as patient is experiacing sob whenever he is having tachycardia(mat) adequate bronchodialtors are given
SOAP notes
DAY 4
21/10/21
Fever chart :

S: : decrease in SOB
No fever episode .
O : Pt is conscious ,coherent, cooperative
Pt has tachycardia
O/E
Pallor +
PR 90 bpm
BP 110/70 mmHg
RR 22 cpm
Temp 98.4 F
GRBS 170 mg/dl
CVS :
Jvp increased
Apex beat in 6 th ICS at MCL
S1 S2 heard
RS :
NVBS +
COARSE CREPTS IN B/L ISA,IAA
P/A :
Soft , non tender
Bowel sounds +
CNS : NAD ,HMF INTACT
A:
DCMP secondary to IHD With MAT ( Multifocal Atrial Tachycardia )
secondary to CAD with COPD with Non healing ulcer of left foot since 10 yrs ( S/p : grafting ? )
P:
1.)Head end elevation upto 30°
2)Oxygen supplementation .Maintain O2 at > 92%
3.)Fuild restriction upto 1 lit / day
4)Salt restriction < 2 g/ day
6.)Inj pantop 40 MG /IV /OD
7.)Tab carvidelol 3.125 mg / po/bd (increased from od to bd)
8 am ......x ......8 pm
8) Tab Dolo 650 mg PO /SOS
9)Nebulisation with ipravent 6 th hrly and budecort 12 th hrly .
10.)Dressing for Left LL ulcer
11) Moniter vitals
12) Strict I/o charting
13) Tab Ecosprin AV /PO/ HS .....75/20
x ...........x..........8 pm
14) Inj Clexane 40 mg / sc / od
15) Inj lasix 40 mg iv/bd

Comments
Post a Comment