15 YEARS OLD MALE PATIENT WITH ACUTE KIDNEY INJURY
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : K. Supriya (9th semester)
Roll number : 53
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
Presenting complaints :
Shortness of breath since 4hrs ,Grade ll -III according to NYHA classification ,associated with orthopnea
Chest pain since 4hrs
This 15 year old male patient ,who is 9th standard student from gurukul school ,Nalgonda , he is a boarding student ,who is staying in hostel from past 5 years ,but due to Corona ,he is at home since 2years.
As he is staying at home since 2years, this history is according to his grand mother .
He is active person and interested in outdoor games,he usually wakes up at around 8am and have breakfast (idly/dosa /wada etc)at 9am ,and play different games with his friends and have lunch(rice &curry) at around 12:30pm ,have some tea in the evng and have dinner(chapathi/ rice) at night 8pm.His diet is mixed but takes very little amount of water intake (like 2-3 glasses in a day).
He is a term child,breast fed upto 1year .
He is a child of parents (third degree consanguineous marriage).no delayed milestones and no physical abnormalities and have good IQ.
HOPI :
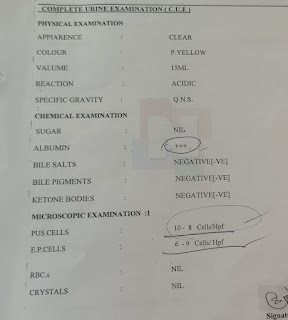
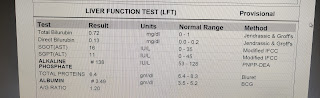
Patient was apparently assymptomatic 1 month ago , then he had vomitings (non bilious with food particles,no blood )at night almost daily upto one week for which he was treated at local hospital and diagnosed with renal problem on evidence from investigation report shown elevated serum urea and creatinine and USG abdomen reports shown bilateral kidney size of 8.1cm with loss of CMD& increased echotexture with grade l RPD changes then he is referred to Hyderabad ,where he undergone 5 series of hemodialysis then came to nalgonda ,again 4 series of hemodialysis done ,actually today he has dialysis session but all of a sudden he developed SOB at night
Shortness of breath is aggravated on supine position ( orthopnea) .and no PND
Chest pain associated with SOB ,which is of dragging type .
No H/O fever,chills & rigor since one month
No H/O decreased urine output , burning micturation ,pedal edema and facial puffiness .
No H/O palpitations and syncopal attacks .
Previous reports :



Past History:
Not a K/C/O diabetes ,Asthma ,TB
Hypertension was diagnosed on diagnosis of renal problem and patient is on Amlodipine 5mg since then .
H/O seizures at age of 2yrs .( Only once till now ),for which he was treated .
Family History :
No H/O renal problems in their whole family .
Personal History:
Appetite -normal
Diet -mixed
Bowel and bladder movements - regular
Sleep - adequate
No allergies and addictions
General Examination:
Patient is conscious, coherent , cooperative
Pallor -present
Icterus -absent
Clubbing-absent
Cyanosis -absent
Lymphadenopathy-absent
Edema -absent
Vitals :
Temperature : afebrile
Pulse rate : 96 bpm
Respiratory rate : 24 cycles /min
BP : 140/100 mm of Hg
SpO2 : 86 % at Room air .
GRBS : 121 mg%
Systemic Examination: CVS
Inspection :
Shape of the chest : elliptical (transverse diameter is more than AP diameter )
Symmetry: bilaterally symmetrical
Position of trachea : central
there is no precordial bulge ,
,no scars and sinuses ,no engorged veins
Palpation :
All inspectory findings are confirmed
Position of trachea is central
Apex beat -at left 5th intercostal space (1cm medial to mid clavicular line)
No thrills .
Auscultation :
S1S2 HEARD
No murmurs
RS :
Bilateral Air Entry - present
Bilateral crepitations heard at IAA and ISA.
No wheeze .
PA:
Soft ,non tender
Bowel sounds +
CNS:
NAD
Investigations :





Tachypnoea :
ECG report :


Provisional diagnosis : Acute Kidney Injury (AKI)
Treatment :
1. Tab Lasix 40mg po/ BID
2. Neb with duolin ,budecort -8th hourly
3.Tab .Zoffer - 4mg po /TID
4. Tab .Nodosis -500mg po /BID
5. O2 inhalation to maintain SpO2
6. Tab orofer AT po /BID
7.STRICT I/O CHARTING
8. BP ,PR,RR CHARTING
9. Tab Rantac 150 mg po /OID

Comments
Post a Comment