45 YEAR OLD MALE PATIENT WITH SEPTIC SHOCK SECONDARY TO LEPTOSPIROSIS
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : K. Supriya (9th semester)
Roll number : 53
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 45 YEAR OLD MALE PATIENT FROM VELUGUPALLY , SURYAPET PRESENTED TO THE CASUALITY ON 2/11/21 WITH THE CHIEF COMPLAINTS OF ;
Fever since 4 days
Body pains since 4 days
Reduced urine output since 3 days
Vomiting yesterday
Hematuria since morning
Black tarry stools since morning
On presentation : patient is hypotensive and dyspnoeic .
This patient ,who is a farmer by occupation ,used to wake up at 5:00 am in the morning ,freshens and go to fileds. He used to have lunch at around 1:30 pm and takes rest for an hour following lunch ,then he goes to work for another 2hrs and return homes by 5:00pm and takes bath and have his meal . Daily he goes out with his friends to have alcohol in the evenings ,then he returns home and have dinner at around 8:00 pm with his wife and 2 children and goes to sleep by 9:00 pm .
He has very good relationships with his family and friends .
Since he works in the farm from morning till eve, until 4 days back ( 29th October 2021 ) when he developed fever along with cough ,headache. He received medications given by the local physician but nothing much changed.
A day or two later he developed muscle pains which he described to be in both his arms and thighs and the fever was back again.
He took medications for one more day
But nothing seemed to improve
Also a new addition to his problems were vomiting
This was when he was taken to local hospital ,where the attenders gave information about the patient being given fluids but they felt that proper care was not being taken and hence they brought the patient to our hospital .
On follow up , we found out that he had passed much less urine than he usually does since the past couple of days and that day he had passed stools which were black in colour.
His wife works as a farmer as well. His wife was previously admitted here with ?meningitis.
HOPI:
Patient was apparently assymptomatic 4years ago ,then he has been experiencing high grade fever, intermittent with no diurnal variation associated with pain in his thigh muscles and arm.
1 year ago he presented to our hospital with the complaints of pain abdomen after which he underwent an abdominal surgery.
Since 4 days , he has High grade fever,which is intermittent,not associated with chills and rigors and
2 episodes of non projectile, non bilious, blood tinged vomiting yesterday .
1 episode of black tarry stool in the morning
Hematuria since morning
Reduced urine output since morning
There is history of change in water source and also contamination of right ankle with rat's urine in his farmlands
Past History:
not a known case of diabetes ,HTN ,Asthma ,epilepsy ,TB
Past surgical history : underwent abdominal surgery (perforation of intestine ).
Personal History:
Appetite : Normal
Diet : mixed
Bowel and bladder movements : decreased urine output and hematuria present.
Addictions : He is an alcoholic since the past 20 years with around 90 ml of whiskey everyday. His last intake of whiskey was 4 days. He smokes around 2 packs of beedi everyday since the past 20 years.
No allergies
General Examination :
Patient is conscious , coherent and cooperative .
Thin built , moderately nourished .
Pallor -present
Icterus - present
Clubbing - present
Subconjunctival hemorrhage - present
Image of right eye showing icterus

Images of left eye showing sub conjuctival haemorrhage


Image showing yellowish discolouration of nails and clubbing

Vitals :
Temperature: Afebrile
PR - 115bpm
RR - 25 cpm
Bp was 60mmhg on palpation
Spo2 - 92% on Room air

Systemic Examination :
Rs :
Bilateral Air Entry -present
Inspiratory crepitations in Bilteral IAA,ISA

4/11/21 xray chest

7/11/21 chest xray

8/11/21 chest xray


CVS:
S1,S2+
JVP -Normal

Per Abdomen -
Soft
Nontender

Investigation findings :
HB - 8 ( outside 2 days back 11g/dl)
TLC - 8400
Plt - 15,000
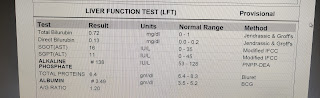
Total Bilirubin - 11
Direct Bil - 7.05
Ast - 327
Alt - 187
Alp - 303
Albumin - 2.4
Serum creatinine - 2.5
Blood urea - 82
Dengue negative
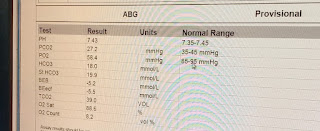
Abg showing metabolic acidosis with PH 7.32
Hco3 - 9
Pco2 - 19
Po2 - 101 with oxygen on 6L of O2
Treatment :
IV fluids (NS ,RL) -75ml /hr
Inj .PAN -40 mg IV /OD
Inj .zofer -4mg IV /TID
Inj .Neomal 1g /IV /80s (if temp > 102°F )
Tab .PCM PO /BD
Inj . Doxycycline 100mg /IV /BD
Inj .ceftriaxone 5g /IV /BD
Inj .NA -DS @10ml /hr
Tab .Udiliv 300mg PO/BD
Syrup .lactulose 15ml /PO /HS
inj thiamine 200mg in 100 ml NS /IV /TID
BP /PR /SPO2 charting Hourly
Strict I/O charting Hourly
Temperature 4th hourly
Provisional diagnosis:
Septic Shock secondary to Leptospirosis
Pyrexia with bicytopenia
Direct hyperbilirubinemia and prerenal AKI
IN CONCERN OF DETAILED FOLLOW UP OF THIS PATIENT : the following SOAP NOTES Obtained from PRASHANT SHARMA sir ( intern)
311/21
In view of low platelet count of 14,000 sdp transfusion is planned.
After doing cross matching a screened unit of sdp is issued to the patient for transfusion after taking consent from the patient attenders.
Post transfusion the platelet count is improved to 35000.
4/11/21
S- patient is complaining of, productive cough with hemoptysis ,
chest pain - non radiating , burning type ,
Increasing on coughing and taking deep inspiration
O- icteric,pallor, subconjunctival hemorrhage
Afebrile
PR-
BP- 110/80 mmhg on Noradrenaline -16 ml /hr
RR- 36/min
Spo2- 99% of
RS- BAE present ,crepts over left infraxillary ,infrascpular regions .
CvS- S1, S2 heard
P/ A soft
Urine output - increased
I/O - 3200/1300 ml
Ecg - showing PR prolongation
A- Septic shock secondary to leptospirosis ( Pre Renal AKI - resolving
Pyrexia with bicytopenia
First degree heart block
Hypoxia + - secondary to pneumonia ?
P- Oxygen supplementation @14 litres/ min to maintain spo2 more than 95%
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring
This case is intubated in view of respiratory failure..on 4/11/21
ABG shows
pO2:-41
FiO2:-60
Patient ET tube blocked with blod clot .
Even after mucomist,ambu and suction saturations weren't improving .
Removed and placed a new tube.
During which patient had Bradycardia ,hypoxia and absent central and peripheral pulses ,
3 cycles of CPR done , patient revived .
Post CPR vitals -
Pupils -
PR-112/ min ,regular
Bp-110/80 mmHg
RS - BAE + , bilateral diffuse crepetations +
CVS-s1 ,S2 heard
Spo2-100% with Fio2-80 %
ABG - severe acidosis mixed metabolic and respiratory -acidosis
Image showing chest xray post reintubation

5/11/21
2 units of FFP is transfused after doing crossmatching.Consent was obtained for transfusion from the patient attenders and transfusion done
Day 3 of mechanical ventilation .
Patient is becoming conscious intermittently ,with eye openings to painful stimuli and verbal commands .
No fever spikes .
O- Pt onmechanical ventilation -AcMV - VC mode
With RR- 33/ min
Peep - 7
VT-400 ml
Fio2-21 %
icteric,pallor, subconjunctival hemorrhage
Pupils - normal size ,non reacting to light
Afebrile
PR-97/ min ,regular
BP- 120/80 mmhg
Spo2- 94% with fio2-21%
RS- BAE present ,bilateral crepts + infraxillary ,infrascpular regions .
CvS- S1, S2 heard
P/ A soft
Urine output - increased
A- MODS- weils syndrome
P-
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring.
Weaning sedation .
Plan to - Shift to CPAP mode
7/11/21
Extubation done at 01:00pm on 7/11/21
Under all aseptic precations,with premedication inj.HYDROCORT 100MG IV STAT and nebulisation with BUDECORT and MUCOMIST , extubation was done. Procedure was uneventful and post extubation vitas are stable.
Bp :120/70mmhg
Pr :108bpm
Spo2 : 98% On 10L of O2
Cvs : s1 s2 heard
RS : BAE present
P/A :soft and nontender
GCS : E4V5M6
Day 1 after extubation
weils syndrome MODS
S- patient is having fever spikes , cough with sputum yellow coloured,non blood stained ,shortness of breath , generalized bodypains .
Yesterday night - patient had one episode of high grade fever with chills ,became tachypneic .
Connected to NIV - CPAP.
O- ABG with high flow oxygen showed Hypoxia ,hence
Patient was on CPAP PC mode overnight
With RR- 33/ min
Peep - 7
Fio2-50%
icteric,pallor, subconjunctival hemorrhage
Afebrile
PR-90/ min ,regular
BP- 130/90 mmhg
RR-37 / min
Spo2- 100% with fio2-80%
RS- BAE present ,bilateral crepts + infraxillary ,infrascpular regions .
CvS- S1,S2 heard
P/ A soft
A-
1-MODS- weils syndrome
2- Ventilator Associated pneumonia ?
P-
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring.
In view of persistent fever spikes ,hypoxia , tachypnea,new radiological opacties -Emperical antibiotic coverage for VAP was started with levofloxacin and vancomycin .
Day wise ABG reports
2/11/21 , 8.36pm

3/11/21 , 9.51 am

4/11/21 , 12.07pm

4/11/21, 1.28pm

4/11/21 , 6.12pm

4/11/21 , 10:23pm

5/11/21 , 08:30am

5/11/21 , 12.18pm

5/11/21 ,5.26 pm

6/11/21 , 3:19 pm

6/11/21 , 11:09 pm

7/11/21, 2:14pm

7/11/21 , 7:41 pm

7/11/21 , 10:34pm


Comments
Post a Comment