27 year old Female with SEIZURES
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : K. Supriya (9th semester)
Roll number : 53
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
27 year old female patient from Nakrekal came to the OPD with the ,
Chief complaints :
1 episode of Generalised tonic clonic seizures
HOPI:
Patient was apparently assymptomatic 12years ago ,then she underwent RTA followed by seizures ,for that she used medication .
8years ago ,She was diagnosed with thyroiditis associated with goitre for which she used carbimazole .
In 2015 - she underwent thyroid surgery ,where one lobe of thyroid is removed and continued on carbimazole
In 2021 -her 2nd lobe of thyroid removed along with parathyroid gland and started on thyronorm 100mcg -she is not on follow up since then .

After thyroidectomy Surgery in 2021 ,patient complaints of parasthesias in B/l lower limbs frequently ,for which she received multiple calcium injections but not relieved of parasthesias .
Now ,since 2 to 3 days she developed parasthesias , giddiness ,generalised weakness for which ,she was taken to local hospital in Nakrekal yesterday (i.e..,31st March at evening 5pm ) .
There ,Patient was started on Tramadol ,Neurobion and NS .
With in No time ,she developed clinching of fists ,frothing and tongue bite (ie..,1 episode of seizure ) followed by 10-15 mints of postictal confusion . Then she was given inj midaz 2CC and inj levipil 1gm IV stat and was referred to our hospital .
She also complaints of excessive thirst .
No H/O fever, altered sensorium ,head ache ,vomitings ,neck pain ,chest pain .
Past History :
not a known case of diabetes ,HTN ,Asthma ,epilepsy ,TB
Personal History :
Appetite : Normal
Diet : Mixed
Bowel and bladder movements : regular
Sleep -adequate
No addictions and allergies
General Examination :
Patient is conscious ,coherent ,cooperative
She is moderately built and moderately nourished
No pallor , icterus ,cyanosis ,clubbing ,lymphadenopathy , edema
Trousseaus sign :
Vitals :
Temp : 98F
Pulse rate : 77bpm
Respiratory rate : 19cpm
Blood pressure: 120/80 mm hg
Systemic Examination :
CNS :
Higher mental functions -intact
Tone -normal
Muscle power -5/5
Reflexes - brisk
Cerebellar signs:
Finger nose test - normal
Dysdiadokinesia -normal
Sensory system - normal
Gait :
CVS :
S1 ,S2 heard
No murmurs
RS:
Normal vescicular breath sounds heard
No crepitations .
PA:
NAD
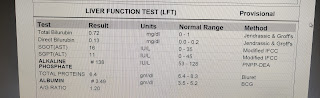
Investigations :








Provisional diagnosis :
SEIZURES due to HYPOCALCEMIA ( POST - PARATHYROIDECTOMY) .
Treatment :


Comments
Post a Comment