16YR OLD MALE PATIENT WITH NOSE BLEEDING
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Name : Supriya .K ( Intern )
Roll Number : 63
A 16 year old male patient, student, was brought to casualty with chief complaints of bleeding from nose since 4 days and fever since 4 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 4 days back and then he developed fever which was high grade, continuous type and associated with chills and rigors. It was relieved temporarily on medications. Patient also had bleeding from nose since 4 days, recurrent type, occurring 2-3 times per day, each episode lasting for 1 hour. Patient also has headache and body pains (back ache*) since two days. Patient has a history of nose bleeding since last 5 years but did not get treated for it.
No history of cold, cough, vomiting.
PAST HISTORY:
No similar complaints seen in the past. Patient is not a known case of Diabetes, Hypertension, Tuberculosis, Asthma, Epilepsy, CVD.
FAMILY HISTORY:
No similar complaints seen in family.
PERSONAL HISTORY:
Diet is mixed
, appetite is normal,
sleep is adequate,
bowel and bladder movements are regular.
No known allergies.
Non smoker and does not consume alcohol.
No H/O intake of any kind of medications.
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative. Well oriented to time, place and person. Moderately built and moderately nourished.
There is no pallor, icterus, cyanosis, clubbing, lymphadenopathy and edema.
Vitals --- BP: 110/70 mmHg PR: 89 bpm Temp: afebrile RR: 18 cpm
SYSTEMIC EXAMINATION:
Cardiovascular: S1, S2 heard; no murmurs Respiratory: NVBS + BAE+ CNS: NAD P/A: Soft, non tender.
PROVISIONAL DIAGNOSIS:
? Dengue Fever ( with thrombocytopenia and NS1Ag Positive with Mild Splenomegaly )
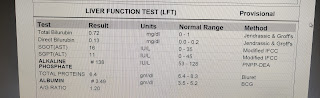
INVESTIGATIONS:
















MANAGEMENT :
I.V fluids- NS & RL for 75ml/hr
T. pan 40mg po/od
Temp monitoring fourth hourly..
Vitals monitoring
SOAP NOTES:
ICU
Day -2
S
Stool passed ,epistaxis 2 episodes in the morning
No Fever spikes
O
Pt is conscious ,coherent , cooperative
Temp: afebrile
BP: 110/70mmHg
PR : 89bpm
RR :18 cpm
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft and nontender
A
DENGUE FEVER WITH THROMBOCYTOPENIA ,NS1 Antigen positive With Mild Splenomegaly
P
1 )IV fluids NS,RL 75ml/ hr
2) T PCM 650 mg PO/OD
3) Temp monitoring 4 th hrly
4) Vitals monitoring

Comments
Post a Comment