This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : Supriya .K ( Intern )
Roll Number : 63
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
35 YR OlD MALE PATIENT , LORRY DRIVER BY OCCUPATION , RESIDENT OF ATTHAMPET ,CAME TO THE OPD WITH THE
C/O Pain abdomen since 10days,
yellowish discolouration of urine since 8 days
Distension of abdomen since 6 days
Bilateral lower limb swelling since 5 days .
HISTORY OF PRESENTING ILLNESS :
Patient was apparently assymptomatic 10days ago and then developed,abdominal pain ,which was insidious in onset and gradually progressive ,which was of dragging type and diffuse, No aggravating factors but relieved on medication and reccured on stoping medication ,but not relieved on leaning forward .
Yellowish discolouration of urine since 8 days, NOT ASSOCIATED with any poor stream ,pyuria ,hematuria ,increased frequency , nocturia ,Burning micturition but decreased urine output present since 5days
Abdominal distension
and bilateral lower limbs edema since 6days,which were insidious in onset and gradually progressive, pitting type of edema over bilateral lower limbs,till knees
Pitting Type Of Edema :
Constipation since 5 days, Not associatied with passage of blood in stool /melena
PAST HISTORY:
No history of similar complaints in the past
K/C/O DIABETES MELLITUS ,which was diagnosed 5 months ago and started on ORAL HYPOGLYCEMIC DRUGS ( pt couldnt remember the drugs names )
N/K/C/O HTN , EPILEPSY ,CAD,CVA ,TB ,ASTHMA
PERSONAL HISTORY:
Sleep - Disturbed since 10days.
Diet - Mixed
Appetite - Disturbed since 6 days
Bowel and bladder movements : IRREGULAR ( decreased urine output and Stools not passed since 5 days )
Addictions : Alcoholic and chronic smoker since 10years
GENERAL EXAMINATION:
Patient is drowsy not coherent and not co operative, moderately built and nourished.
Vitals at presentation
Temp : Afebrile
BP: 110/80mmHg
PR: 86bpm
RR: 20cpm
SpO2 : 98%
Pallor - absent
Icterus - present
Cyanosis - absent
Clubbing - absent
Lymphadenopathy : absent
Edema : Present till knee level and of pitting type
PER ABDOMEN
Patient was examined after taking consent in a well lit room
ON INSPECTION
Abdomen is distended
umbilicus is inverted
Skin over abdomen is stretched and shiny
No visible pulsations
Engorged veins - Present
PALPATION :
all inspectory findings confirmed
No rise of temperature and tenderness
No guarding and rigidity
No hepatomegaly and Splenomegaly
PERCUSSION :
Shifting dullness - Present
Fluid thrills - Present
Puddle sign cannot be elicited ,as pt is not cooperative
AUSCULTATION :
Sluggish bowel sounds are heard
No bruits
CVS : S1 and S2 heard
no murmurs
CNS: No flapping tremors( Asterexis )
(Apraxia cannot be elicited as pt is not cooperative )
Apraxia Charting after 5 days of Hospital Stay : (19/12/22)
RS : bilateral air entry is present
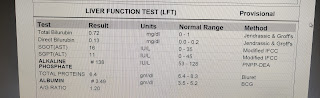
INVESTIGATIONS:
ASCITIC TAP DONE and fluid sent for analysis :
ABG :
CT scan : Showing Calcifications:

Chest Xray:
Thyroid profile:
T3 - 0.60
T4 - 10. 21
TSH - 9.27
USG REPORT:
Enlarged liver with altered echotexture s/o CLD
gall bladder edema with sludge
Gross ascitis
Provisional Diagnosis :
Decompensated Cirrhosis with Portal Hypertension (High SAAG low protein )
Hepatic Encephalopathy Grade I
Alcohol dependence Syndrome
Chronic pancreatitis
Sub Clinical Hypothyroidism
MANAGEMENT:
) IV fluid NS 50 ml /hr
2) inj lasix 40mg IV /BD
3) T. Aldactone 50mg RT /OD
5) Syp . Lactulose 15ml RT /TID
6) Salt and fluid restriction ; Salt < 2gm /day , fluid < 1.5 lit /day
7) inj 3 amp KCL in 500ml NS over 5 hrs
8) Weight and abdominal girth daily
9) GRBS monitoring 2nd hrly
10) vitals monitoring 4th hrly
12) inj .Thiamine 200mg IV /BD
13) 3-4 egg whites /day
14) protein X powder 3-4 scoops in glass of milk RT/TID
SOAP NOTES:
ICU
BED -1
Day -2
Unit -3
S
Stool passed +
No Fever spikes
O
Pt is drowsy ,confused ,non cooperative
Temp: 98.6 F
BP: 110/70 mmHg
PR : 88bpm
RR : 16cpm
GRBS : 87 mg /dl
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+ , GCS : E4V4 M6
P/A : Soft and non tender
A
CHRONIC LIVER DISEASE SECONDARY TO ALCOHOL with hypokalemia and Thrombocytopenia
P
1) IV fluid NS 50 ml /hr
2) inj lasix 40mg IV /BD
3) T. Aldactone 50mg RT /OD
5) Syp . Lactulose 15ml RT /TID
6) Salt and fluid restriction ; Salt < 2gm /day , fluid < 1.5 lit /day
7) inj 3 amp KCL in 500ml NS over 5 hrs
8) Weight and abdominal girth daily
9) GRBS monitoring 2nd hrly
10) vitals monitoring 4th hrly
12) inj .Thiamine 200mg IV /BD
13) 3-4 egg whites /day
14) protein X powder 3-4 scoops in glass of milk RT / TID
ICU
BED -1
Day -3
Unit -3
S
Stool passed +
No Fever spikes
O
Pt is drowsy but arousable
Temp: 98.6 F
BP: 120/80 mmHg
PR : 88bpm
RR : 16cpm
GRBS : 182mg /dl
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+ , GCS : E4V4 M6
P/A : Soft and non tender
A
CHRONIC LIVER DISEASE SECONDARY TO ALCOHOL
ALCOHOL DEPENDENCE SYNDROME
DIRECT HYPERBILIRUBENEMIA , HYPOKALEMIA
P
1) T. Aldactone 50mg PO /OD
2)inj. Vit -k 10 mg IV/OD over 10 min
3)syp. potklor 15 ml in 1 glass of water PO/ TID
4)inj.Thiamine 200 mg IV/ BD
5)3_4 egg whites/ day
6)GRBS monitoring 2nd hrly
7) vitals monitoring 4th hrly
8)protein X powder 3-4 scoops in glass of milk RT / TID
ICU
BED -1
Day -4
Unit -3
S
Stools passed
No fever spikes
O
PATIENT IS DROWSY AND AROUSABLE
Temp: afebrile
BP: 110/60mmHg
PR : 82bpm
RR : 18cpm
GRBS-221GM/DL
I/O :1000/ BEDWET
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN
A
CLD SECONDARY TO ALCOHOL
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
K/C/O DM2 SINCE 6YRS
HYPOKALEMIA(RESOLVED)
P
IV FLUIDS
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG RT OD
POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML RT TID
3-4 EGG WHITES
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 6TH HOURLY
GRBS 7.PROFILE
ICU
BED -1
Day -5
Unit -3
S
Stools passed
No fever spikes
O
Patient is drowsy and responding to only pain
Temp: afebrile
BP: 100/80mmHg
PR : 86bpm
RR : 18cpm
GRBS-Charting :
12AM : 135 mg/dl
2AM : 165 mg/dl
6AM : 135 mg/dl
8AM : 178 mg/dl
I/O :1000/ BEDWET
GCS score at 9:30 am : E4V2M5
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
CLD SECONDARY TO ALCOHOL DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
HEPATIC ENCEPHALOPATHY (GRADE 3 )
K/C/O DM2 SINCE 6YRS
HYPOKALEMIA(RESOLVED)
P
IV FLUIDS
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG RT OD
POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML RT TID
3-4 EGG WHITES
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 6TH HOURLY
GRBS 7.PROFILE
ICU
BED -1
Day -6
Unit -3
S
stools passed (2 times )
No fever spikes
O
patient is oriented to place ,person
Temp: afebrile
BP: 110/70mmHg
PR : 84bpm
RR : 18cpm
GRBS-Charting :
8AM : 178 mg/dl - 4U HAI
10AM: 135 mg/dl
2PM : 209 mg/dl - 7U HAI
7PM: 136 mg/dl
8PM : 198mg/dl - 6U HAI
10PM : 135 mg /dl
2AM : 96 mg/dl
8AM : 158 mg/dl - 6U HAI
GCS score at 8:15 AM : E4V5M6
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
K/C/O DM2 SINCE 6YRS
HYPOKALEMIA(RESOLVED)
P
IV FLUIDS - 3 . NS - 50ML/HR
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG RT OD
SYP POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML RT TID
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 4TH HOURLY
GRBS 6TH HRLY MONITORING
FREQUENT CHANGE IN POSITION 4TH HRLY
ICU
BED -1
Day -7
Unit -3
S
stools passed (2 times )
No fever spikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 120/70mmHg
PR : 74bpm
RR : 18cpm
GRBS-Charting :
8AM : 158 mg/dl - 6U HAI
10AM: 182mg/dl
2PM : 185mg/dl - 6U HAI
4PM : 282 mg/dl
8PM : 275 mg/dl
12AM : 138 mg /dl
2AM : 96 mg/dl
8AM : 148 mg/dl - 6U HAI
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED
ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
HEPATIC ENCEPHALOPATHY -GRADE I
BED SORE -I
K/C/O DM2 SINCE 6YRS
REFRACTORY HYPOKALEMIA(RESOLVED)
P
IV FLUIDS - 3 . NS - 50ML/HR
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG RT OD
SYP POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML RT TID
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1 GLASS OF WATER
VITALS MONITORING 4TH HOURLY
GRBS 6TH HRLY MONITORING
EARLY AMBULATION
AMC
BED -2
Day -8
Unit -3
S
stools passed (2 times )
No fever spikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 110/70mmHg
PR : 92bpm
RR : 18cpm
GRBS:
8AM : 148mg/dl - 6U HAI
2PM : 112mg/dl
8AM : 166 mg/dl - 6U HAI
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
HEPATIC ENCEPHALOPATHY -GRADE I
BED SORE -I
K/C/O DM2 SINCE 6YRS
MILD HYPOKALEMIA,THROMBOCYTOPENIA
SUB CLINICAL HYPOTHYROIDISM
P
IV FLUIDS - 2 . NS - 50ML/HR
INJ MONOCEF 1GM /IV BD
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG RT OD
SYP POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML RT TID
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 4TH HOURLY
GRBS 6TH HRLY MONITORING
EARLY AMBULATION
AMC
BED -2
Day - 9
Unit -3
S
stools passed (2 times )
No fever spikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 120/70mmHg
PR : 88bpm
RR : 18cpm
GRBS:
8AM : 166 mg/dl - 6U HAI
2PM : 155 mg/dl - 6U HAI
8PM : 202 mg/dl
8AM : 121 mg/dl - 6U HAI
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
HEPATIC ENCEPHALOPATHY -GRADE I
BED SORE -I
K/C/O DM2 SINCE 6YRS
MILD HYPOKALEMIA,THROMBOCYTOPENIA
SUB CLINICAL HYPOTHYROIDISM
P
IV FLUIDS - 2 . NS - 50ML/HR
INJ MONOCEF 1GM /IV BD
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG RT OD
SYP POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML RT TID
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 4TH HOURLY
GRBS 6TH HRLY MONITORING
EARLY AMBULATION
AMC
BED -2
Day - 10
Unit -3
S
stools passed
No fever spikikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 100/ 70mmHg
PR : 102bpm
RR : 18cpm
GRBS:
8AM : 121 mg/dl - 6U HAI
2PM : 117mg/dl - 6U HAI
8PM : 121mg/dl - 6U HAI
8AM : 98 mg/dl - 4U HAI
I/O : 1100/900ml
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
HEPATIC ENCEPHALOPATHY -GRADE I
BED SORE -I - Resolved
K/C/O DM2 SINCE 6YRS
MILD HYPOKALEMIA,THROMBOCYTOPENIA
SUB CLINICAL HYPOTHYROIDISM
P
INJ MONOCEF 1GM /IV BD
INJ THIAMINE 200MG IV BD
T. ALDACTONE 50MG PO/ OD
SYP POTKLOR 10ML IN 1 GLASS OF WATER TID
SYP.LACTOLOSE 15ML PO/BD
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 4TH HOURLY
GRBS 6TH HRLY MONITORING
EARLY AMBULATION
AMC
BED -2
Day - 11
Unit -3
S
stools passed
No fever spikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 100/ 80 mmHg
PR : 96bpm
RR : 18cpm
GRBS:
8AM : 98 mg/dl - 4U HAI
2PM : 150 mg/dl - 6U HAI
8PM : 202 mg/dl - 6U HAI
2AM : 173 mg/dl
8AM : 139 mg/dl - 6U HAI
I/O : 1100/1050ml
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION (HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS
HEPATIC ENCEPHALOPATHY -GRADE I
BED SORE -I - Resolved
K/C/O DM2 SINCE 6YRS
MILD HYPOKALEMIA,THROMBOCYTOPENIA(RESOLVING)
SUB CLINICAL HYPOTHYROIDISM
P
T. ALDACTONE 50MG PO/ OD
T. THIAMINE 100MG PO/BD
SYP POTKLOR 15ML IN 1 GLASS OF WATER
PO/ TID
SYP.LACTOLOSE 15ML PO/OD/HS
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 6TH HOURLY
GRBS 6TH HRLY MONITORING
EARLY AMBULATION
AMC
BED -2
Day - 12
Unit -3
S
stools passed (2 episodes)
No fever spikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 130/ 80 mmHg
PR : 96bpm
RR : 18cpm
GRBS:132 gm/dl
I/O:1000/750 ml
CVS : S1 S2 +
RS : BAE +
CNS :NAD ,HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS.SUB CLINICAL HYPOTHYROIDISM
HEPATIC ENCEPHALOPATHY -GRADE I
BED SORE -I - Resolved
K/C/O DM2 SINCE 6YRS
MILD HYPOKALEMIA,THROMBOCYTOPENIA(RESOLVED)
P
T. ALDACTONE 50MG PO/ OD
T. THIAMINE 100MG PO/BD
SYP POTKLOR 15ML IN 1 GLASS OF WATER PO/ TID
SYP.LACTOLOSE 15ML PO/OD/HS
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
3-4 EGG WHITE / DAY
VITALS MONITORING 6TH HOURLY
GRBS MONITORING 6 TH HOURLY
WARD
Day - 13
Unit -3
S
Stools passed (2 times )
No fever spikes
No thrombophlebitis
O
patient is conscious,coherent , cooperative
Temp: afebrile
BP: 120/ 80 mmHg
PR : 72bpm
RR : 16cpm
GRBS:
8 AM:132 mg/dl -6 U HAI
2 PM: 160 MG / DL -6 U HAI
8 PM: 158 MG/ DL-6U HAI
2 AM: 163 MG/ DL
8 AM:160 MG/ DL -6 U HAI
I/O:1200/1100 ml
ABDOMINAL GIRTH : 39.5CMS
WEIGHT : 67.7 KGS
CVS : S1 S2 +
RS : BILATERAL AIR ENTRY +
CNS : NAD, HMF+
P/A : Soft , ENGORGED VEINS , DISTENDED ABDOMEN present
MILD HYPOKALEMIA, THROMBOCYTOPENIA ( resolved )
A
DECOMPENSATED CIRRHOSIS WITH PORTAL HYPERTENSION(HIGH SAAG LOW PROTEIN)
DIRECT HYPERBILIRUBINEMIA.
CHRONIC PANCREATITIS.SUB CLINICAL HYPOTHYROIDISM
HEPATIC ENCEPHALOPATHY -GRADE I(RESOLVED)
BED SORE -I - Resolved
K/C/O DM2 SINCE 6YRS
P
T. ALDACTONE 50MG PO/ OD
T. THIAMINE 100MG PO/BD
SYP POTKLOR 15ML IN 1 GLASS OF WATER PO/ TID
SYP.LACTULOSE 15ML PO/OD/HS
3-4 EGG WHITES /DAY
PROTEIN X POWDER 3,4 SCOOPS IN 1GLASS OF WATER
VITALS MONITORING 6TH HOURLY
GRBS MONITORING 6TH HOURLY





























Comments
Post a Comment