60YR OLD MALE PATIENT WITH HEAD ACHE AND NECK ACHE
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Name : Supriya .K ( Intern )
Roll Number : 63
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
60YR OLD MALE PATIENT, RESIDENT OF NARKETPALLY , DAILY WAGE WORKER BY OCCUPATION CAME TO THE OPD WITH
Chief complaints of ;
Neck pain since 6 days
Headache since 6 days
B/L shoulder pain since 6 days
Blurring of vision since 1 year
Patient was apparently asymptomatic 6days ago,then ,he developed headache over B/L temporal region and occipital region ,which is of half n hour duration ,episodic ,no aggravating factors but relieved on medication ,not associated with nausea, ,vomiting ,photophobia ,phonophobia .
Then he developed Neck pain ,which is of dragging type ,diffuse and associated with B/L Shoulder pain
H/O blurring of vision since 1 year
H/O RTA 15 years ago ,which lead to the Fracture of Right sided Tibia , Right sided knee joint and Right sided Radial bone fracture (UNDERWENT SURGERY )and




Head ache started since then (as his head got hit to the ground )which was on and off and dull aching ,diffuse and pain increased in intensity since 6 days and associated with neck pain and bilateral shoulder pain but there was NO H/O Fracture to the Skull not associated with abrasion ,contusion or lacerations over the head . On Radiological examination ,which was done before ( CT scan & MRI - No abnormality detected ).
No Deviation of Mouth
No Weakness of limbs
No H/O chest pain
No H/O palpitations
No H/O SOB
K/C/O Hypertension ,which was diagnosed 7 days ago ( used atenolol as medication )
N/K/C/O DM II , TB , Epilepsy,Asthma ,CVA ,CAD
PERSONAL HISTORY :
Appetite : Normal
Diet : Mixed
Sleep : adequate
Bowel and bladder movements: regular
Addictions: Occasional alcoholic , Smoking since 45years ( Chutta - 4/ day )
Allergies : No allergies
GENERAL EXAMINATION:
Patient is conscious ,coherent , cooperative, Moderately Built and Moderately Nourished .
Temp: Afebrile
BP : 190 /100 mmHg
PR : 80bpm
RR : 20cpm
Pallor : absent
Icterus : absent
Cyanosis: absent
Clubbing : absent
Lymphadenopathy : absent
Edema : absent
SYSTEMIC EXAMINATION :
CVS :
INSPECTION:
Shape of chest- bilaterally symmetrical
Trachea - central
No visible pulsations
No scars,sinuses or dilated veins
PALPATION :
No thrills,parastrenal heaves
AUSCULTATION :
s1,s2 are heard
No murmurs
No raised jvp.
RS : BAE +
CNS : NAD and HMF +
P/A : Soft and Non tender
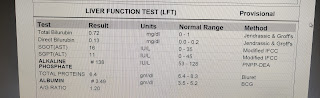
INVESTIGATIONS:










USG : ABDOMEN:




PROVISIONAL DIAGNOSIS :
HYPERTENSIVE URGENCY (DENOVO DIAGNOSED 7DAYS AGO FROM DAY OF ADMISSION)
CERVICAL SPONDYLOSIS .
MANAGEMENT:
T. Nicardia 20mg PO / Stat
T. Cinod 10mg PO /stat
T. Telma H + T. cinod 10/40 mg PO /OD
BP monitoring 4th hrly
Vitals monitoring 6th hrly
( Pt came to OPD ,his BP value recorded as 190/100 mmHg ,then Tab. NICARDIA 20 mg given , after 30 minutes his BP value recorded as 170 /100 mmHg
Then , Tab.CINOD 10mg given at around 9: 20PM ,then his BP value recorded as 140/80 mmHg .
BP CHARTING:

SOAP NOTES :

Comments
Post a Comment